Trigger Warning: This article contains descriptions of suicide.
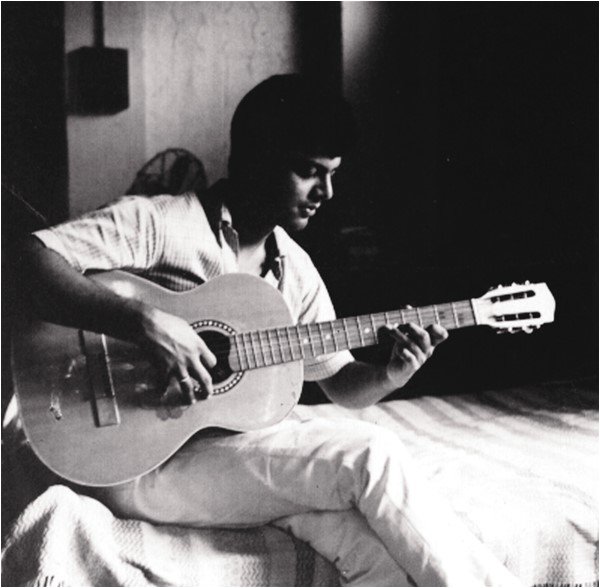
Guru Dutt, one of India’s most revered filmmakers, would have turned 100 this year.
Dutt is celebrated for creating masterpieces like Pyaasa and Kaagaz Ke Phool (Hindi for ‘Parched’ and ‘Paper Flower’, respectively) that inspired generations of filmmakers. Yet, as his biographer, I was struck not just by his cinematic genius, but by the constant, silent struggle he endured as his mental health disintegrated parallelly to the release of some of his best work. In this milestone centenary year, it feels essential to confront the shadows that long lingered behind the brilliance of his work, a pain buried for too long. In the high-stakes world of filmmaking, particularly in South Asia, the same shadows persist even today—mental health remains a glaring blind spot. But first, let’s return to Dutt’s unfinished story.
As a biographer, I was curious about what troubled the auteur, who kept trying to end his life until he succeeded at the young age of 39. Dutt’s younger sister and artist, the late Lalitha Lajmi, had witnessed his life and times at close quarters, and shared vivid memories while collaborating for my biography on Dutt.

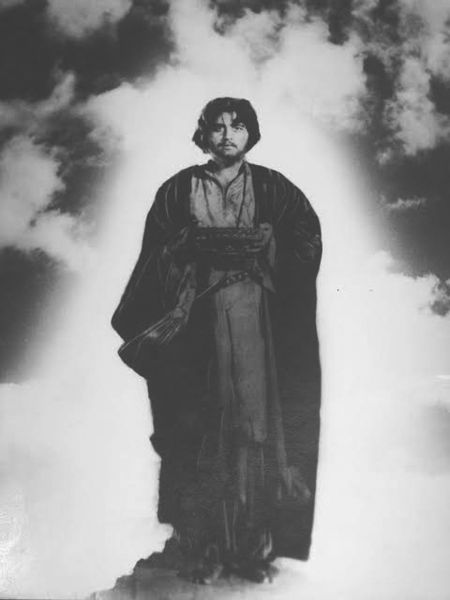
Left: Guru Durr in Pyaasa (1957); Right: Guru Dutt and Abrar Alvi at the premiere of Pyaasa
It was in 1956 when Dutt’s dream project Pyaasa (the only Hindi film to make it to the ‘100 Greatest Films of All Time’ list by Time magazine) was nearing completion. This is when news broke about Dutt’s attempted suicide. The 31-year-old had swallowed a copious amount of opium. In my book Guru Dutt: An Unfinished Story, Lajmi remembered: “I knew he was in turmoil… When the news came, we were stunned. I remember his body had turned cold and his vision had blurred. He kept repeating, ‘I’m becoming blind, I can’t see…’”
People close to Dutt could never really know if this move was due to skirmishes in his personal life, mood disorder, philosophical reasons or just poor impulse control. Neither did they seek professional help after he was discharged from the hospital. With scarce conversations around a socially stigmatised topic and big money riding on the magnum opus Pyaasa, Dutt found little time to address what was happening to him.
The rejection of the world and life itself was a prominent theme of Pyaasa. The movie became a major commercial and critical success and catapulted Dutt into stardom. Next came the brooding, quasi-autobiographical Kaagaz Ke Phool, which mirrored Dutt’s own story, his unhappy marriage and his confusing relationship with his muse. It eerily ends with the death of the protagonist, a filmmaker, after failing to come to terms with his acute loneliness and doomed relationships. Kaagaz Ke Phool, now considered a classic, was rejected by audiences when it was released in 1959. It broke his heart and confidence so much that he never officially directed a film after that. “He was sleepless and in a terrible state of mind. His constant refrain was: ‘I think I will go crazy,’” Lajmi told me in my book.

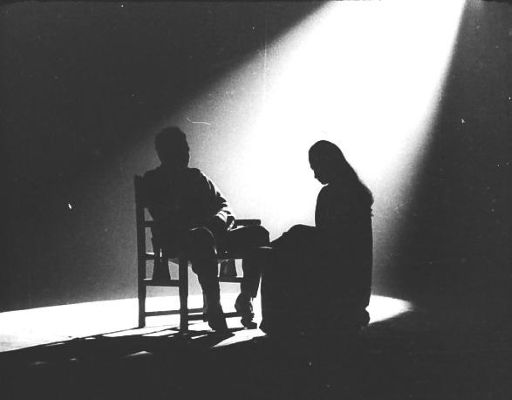
(Left) A shot from Kaagaz Ke Phool (1959) filmed inside Vauhini Studious, Madras; (Right) Kaagaz Ke Phool (1959): The rise of the director. Fans lining up for autographs.
The celebrated cinematographer VK Murthy recalled a heartbreaking conversation with Dutt in an interview: “Kaagaz Ke Phool upset him very much… he (would quote) a line from Pyaasa: Agar yeh duniya mujhe mil bhi jaye to kya hai? (Even if I get the world, what does it matter?) I asked him why he said that. ‘Mujhe waise hi lag raha hai. Dekho na, mujhe director banna tha, director ban gaya; actor banna tha, actor ban gaya; picture achcha banana tha, achche bane. Paisa hai, sab kuch hai, par kuch bhi nahi raha (I feel this way. I wanted to become a director, I became one; I wanted to become an actor, I became one; I wanted to make good films, I made them. I have money, I have everything, yet I have nothing).”
Lajmi recalled that at that time, the family believed that Dutt had internalised the serious characters of his dark films leading to his inner turmoil. But what was even more tragic was that his suffering was evident, yet neither he nor those around him sought professional intervention as mental health awareness was simply nonexistent in 1960s India.


(Left) Chaudhvin Ka Chand (1960): Guru Dutt’s biggest commercial success ever; (Right) Guru Dutt and Waheeda Rehman in a still from Sahib, Bibi Aur Ghulam (1963)
Lajmi recalled: “Even though his next Chaudhvin Ka Chand was a huge success, Dutt’s melancholy persisted. By Sahib Bibi Aur Ghulam, which won the President’s Medal, he appeared to be in deep depression—though never formally diagnosed.”
Soon after, in a shocking move, on his birthday in 1963, he demolished his own bungalow, his dream house in Mumbai’s Pali Hill neighbourhood. Then one night, he swallowed 38 sleeping pills – his second attempt at suicide.
“The second time, it was an overdose of sleeping pills. His body had gone completely cold. He was unconscious for three days,” Lajmi recalled in Guru Dutt: An Unfinished Story, adding he never spoke with her about his repeated suicide attempts, “Sometimes he used to call me. I would rush to him even in the middle of the night. But he would sit in silence. I felt he wanted to say something. But he never really confided. Never. He was disturbed.”
After he survived the second suicide attempt, his friend and writer of Sahib, Bibi our Ghulam, Bimal Mitra is quoted him in his book, Bindira (Sleepless), asking him: “You have fame, you have wealth, you have the adoration of the masses. You possess all that most people crave for! Why are you so dissatisfied with life?” Dutt replied, “I am not dissatisfied with life, I am dissatisfied within myself.”
‘Madness’ and Media in South Asia
The media industry of the 1960s India turned Dutt’s pain into salacious gossip, reducing his suicide attempts to a failed love affair and a broken marriage, even blaming his wife, Geeta Dutt, for his condition.


1) Geeta Dutt—The star singer who married a struggling film-maker; 2) Guru and Geeta Dutt at their wedding; 3) Geeta with a young Tarun Dutt, their son.
Geeta told me: “I was much younger than him and in those days, no one really talked about such things. In 1963, as suggested by his doctor, we also called a psychiatrist but he charged Rs 500 for a visit. My brother Atmaram laughed that he was ‘just talking’ with Guru and he is so expensive. We never called the psychiatrist again.”
Dutt’s final rejection of the world came swiftly. On October 10, 1964, he was found dead in his room, a glass of pink liquid — sleeping pills, Sonaril, crushed and dissolved in water — on the side table.
Left: Shooting still from K. Asif’s Love and God. Dutt was playing Majnu but passed away before completing the film. This was supposed to be K. Asif’s next mega project after Mughal-E-Azam.
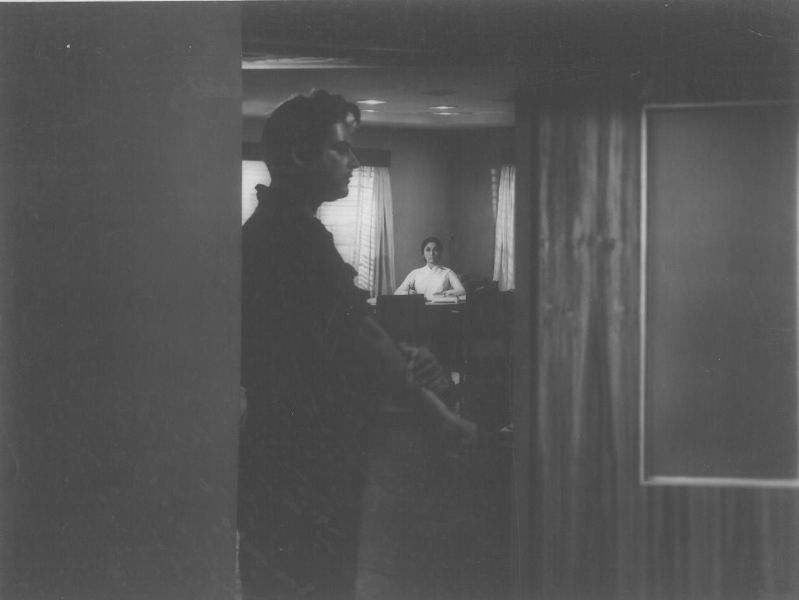
Right: Guru Dutt’s final scene, the film is Baharen Phir Bhi Aayengi (1966). Playing a reporter in the film, he resigns from his job. He throws his resignation letter on the table and tells his editor (Mala Sinha), “Whether you accept it or not, this is my resignation. I am going.”
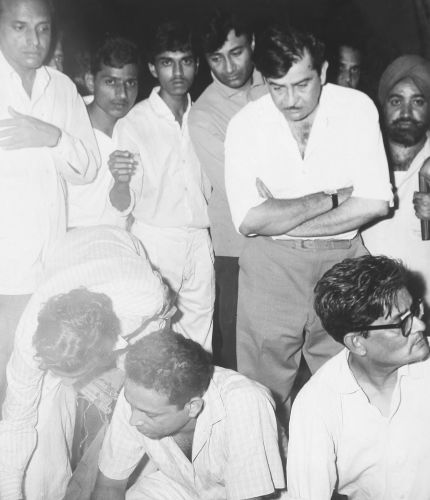
Left: Guru Dutt and Waheeda Rehman in Kaagaz Ke Phool (1959); Right: Indian actors Dev Anand and Raj Kapoor at Guru Dutt’s funeral
Once again, the media reduced his death to a tragic romance, putting the blame between his wife or his muse, weaving it into legend. But no one addressed the crucial question around his mental health.
In fact, even the six decades since Dutt’s death, there’s been little effort to address mental health in the industry.
“When it comes to mental health, it is very much real to have a sense of perceived discrimination, stigma and hesitancy in seeking help leading to delayed intervention,” Dr Samir Parikh, a psychiatrist and director of the Department of Mental Health and Behavioural Sciences at Fortis Healthcare, tells Asian Dispatch. “A surgeon, a journalist, an athlete and a politician – they all have different kinds of stresses. But if you’re in an industry where ‘How many people constantly appreciate your work?’ is at the core of what you do than the peoples’ involvement, it also becomes a part of the entire process. Just because you become accustomed to adulation of people does not mean you don’t feel human emotions or you do not feel hurt. It is even more exaggerated.”
Dutt’s struggles weren’t the only one within the Indian film industry. The six pivotal decades since his death have been lost opportunities for change.
In the 1980s, when leading actress Parveen Babi was reportedly diagnosed with schizophrenia, the media industry didn’t grasp her ordeal. In fact, it sexed up her “madness.” Cover stories analysed her collapses with voyeuristic relish, quoting lovers, producers and directors bemoaning their loss instead of her suffering.
In several headlines such as “What drove Parveen to another breakdown? 12 concerned men reveal the real story” (Star & Style, Sept 16-29, 1983) and “EXPOSED! A common factor in Babi’s three breakdowns” (Stardust, October 1983), the narrative wasn’t of a woman battling a frightening illness; it was one of how her illness intruded upon others. Filmmaker Vijay Anand is quoted by the 1983 edition of Star & Style as saying: “There’s no doubt her illness is a genetic problem. I personally feel she should give up working and settle down.”
Piece on Parveen Babi’s ‘breakdowns’ in Star & Style magazine, 1983. Sourced from archives by Usman.
“The treatment of Parveen Babi was widely documented and even today you’ll see people using similar language very casually — mental illnesses as a slur or insult — which really can be hurtful,” Amrita Tripathi, the founder-editor of The Health Collective told Asian Dispatch. Babi’s reported schizophrenia made her an outcast in the world she once ruled. Isolated and forgotten, she withdrew first from stardom, then from life—until she died alone in 2005.
A decade later, in the 1990s, another Bollywood actor Raj Kiran disappeared, owing to his battle with depression. In 2011, there were news stories of him being sighted in a mental facility in Mumbai and later in Atlanta. Thankfully, his story lacked the tabloid frenzy of Babi’s. But the end was the same: Silence, neglect and an industry that simply looked away.
In Pakistan, too, the silence around mental health has been deafening. Waheed Murad, the nation’s beloved “chocolate hero,” reportedly spiralled into depression as his career faded. Yet, neither he nor anyone close to him acknowledged the issue. When he died in 1983, the media fixated only on the question: Was it suicide or a heart attack? Was he depressed or simply heartbroken by failure? Never once addressing the possibility that mental illness might have played a role.
Years later, Pakistan’s famous film and TV actress in the 1970-80s, Roohi Bano’s battle with schizophrenia met the same fate. Senior Pakistani journalist and film critic Omair Alavi told me: “In South Asia, particularly in India and Pakistan, ‘hero worship’ elevates actors to near-mythical status. But when the spotlight shifts and audiences move on, the descent can be brutal. For stars already battling mental health struggles, this pressure can be devastating.”
When Murad died at 45, media narratives fixated on his alleged suicide, Alavi adds, framing it as a failure to cope with fading stardom rather than a lack of mental health support. “Bano’s tragic case was covered with almost no empathy for her schizophrenia delving more into tabloid-style gossip,” he says.
Different countries and different people, but same stories and the same lack of empathy. In all these cases, the underlying issue—mental health—was buried beneath scandal and silence. Sometimes, the non-A listers escaped the wrath of being in public glare. Was it a blessing in disguise?
In another South Asian country, Bangladesh, actor Salman Shah, hailed as the “First superstar of modern Dhallywood,” was found dead in 1996 amid rumours ranging between a family feud to an affair. Shah’s ex-wife, Samira Haq, later revealed that there were multiple suicide attempts. “He (Imon) was mentally suicidal by nature. He attempted suicide three times before his death. You can check the records of Metropolitan Hospital,” she told Bangladeshi publication, Daily Sun.

Left: Waheed Murad, Pakistan’s beloved ‘chocolate hero’. Photo: Wikimedia Commons; Right: Salman Shah, the first superstar of Bangladeshi cinema. Photo: IMDB
{kind=link}
In Nepal too, the tragic death of film actor Saruk Tamrakar in 2023 sparked a debate on mental health in the filmmaking community there. “As a journalist covering celebrities, I’ve observed how, in Nepalese society, wealth and fame often overshadow personal struggles. Tamrakar’s passing was a shock, but had he spoken out, many might have dismissed him as attention-seeking. That’s also a harsh reality celebrities face when dealing with mental health issues,” says Anish Ghimire, culture and lifestyle editor at The Kathmandu Post.
In South Asian societies, even hinting that a star struggles with mental health is deemed a career-ending move. British-Indian actress Jiah Khan, who acted in big Bollywood films like Ghajini, Housefull and Nishabd, died by suicide on June 3, 2013, at a very young age of 25. Her six-page suicide note hinted at a young woman’s silent battle with depression under tremendous personal and professional pressure.
“The perception problem with mental health issues in India is, firstly, an absolute denial, even in private, let alone public,” senior film critic and newspaper editor Mayank Shekhar told Asian Dispatch. “This problem grows all the more with the rich or accomplished or famous—the popular argument being, since they’re doing so well, what could they be suffering from, say, depression for? This altogether ignores the dimensions of darkness and disease.”
Shekhar adds: “With cinema heroes, perhaps, it gets worse, because they also have a public/screen image to zealously project and protect.”
A Space for Change
Surprisingly, the past decade saw a shift. Mental health conversations slowly entered the mainstream, chipping away at long-held stigma. A pivotal moment came in 2015 when Bollywood star Deepika Padukone openly shared her battle with clinical depression.
“Being able to define my condition was an important first step on my path to recovery,” she told The New York Times, recalling how she first experienced symptoms in 2014 after fainting from exhaustion. Her admission was unprecedented in an industry where vulnerability was rarely acknowledged, let alone discussed and it sparked nationwide discussions. Even Hrithik Roshan, Bollywood’s ‘greek god’, opened up about dealing with feelings of depression saying he “was dying” during the filming of his action film War (2019): “I was completely lost, and that’s when I knew that I needed to make a change in my life.”
Then in 2020, Bollywood actor Sushant Singh Rajput’s tragic death in 2020, during the COVID-19 pandemic, pierced through that illusion of progress, and showed how little has changed since Dutt’s time.
Rajput’s death spiralled into sensationalism as the media, the film industry and even many mental health professionals – hungry for publicity – turned his death into a spectacle. His struggle with mental health was dissected like a mystery to be solved or, worse, a dark secret to be exposed. For months, news outlets reduced the complexities of mental illness to simplistic narratives that fed into societal prejudices. Such voyeurism surrounding his death undid years of awareness and empathy, casting mental health once again into the realm of ridicule. This coverage dragged the issue of mental health back into the realm of shame and speculation.
“While there is no doubt (even anecdotally) that awareness about mental health challenges has improved, there is so much sensationalism in our media coverage; which the tragic Rajput case makes evident,” Tripathi, from The Health Collective, says. “There are clear guidelines for reporting on suicide, which are meant to protect against suicide contagion or the Werther effect. It’s beyond troubling that media organisations, journalists and nowadays even ‘influencers’ choose not to follow them or even remain unaware or oblivious to the damage they may be causing.”
She adds: “There is a need to educate ourselves and others on the responsibility we bear towards each other and especially the most vulnerable — the first principle should be to do no harm.”
In recent years, more South Asian stars like Mahira Khan, Meesha Shafi, Shraddha Kapoor, Imran Khan, Alia Bhatt, Arjun Kapoor, Imran Abbas, and others have bravely opened up about their battles with anxiety, depression, and mental health.
Tripathi says that since the pandemic, people – at micro and macro levels – have more awareness and conversations about mental health. “I do believe young people are at the forefront of this— mainstreaming and ‘normalising’ the conversation around mental illness and not judging each other for seeking help when it’s needed,” she says.
Popular cinema and stars in South Asia hold immense influence, shaping perceptions across both the masses and the elite. In 2016, a standout example from Bollywood emerged, called Dear Zindagi, featuring Shah Rukh Khan — arguably the subcontinent’s biggest star — as a charming psychiatrist Dr Jehangir Khan, alongside Alia Bhatt as a young woman seeking therapy. In his paper titled ‘Mental illness in Indian Hindi Cinema’, Ramakrishna Biswal from the National Institute of Technology, Rourkela, had noted how the “depiction of the mental health professional, mainly psychiatrist, in films such as Damini (1993), Dilwale (1994), and Kyon Ki (2005) were shown to be Mr Evil, unprofessional, insensitive, unscientific, apathetic, comic fillers and boundary violators.”
“[Dear Zindagi broke that pattern and] is the first of its kind to correctly show the therapeutic relationship between the mental health professional and the patient,” Biswal told Asian Dispatch.
When A-list actors normalise conversations around mental health on screen, it paves the way for real change. “The only way to advance mental health as a cause is for public figures—those who are followed and respected—to consistently speak about it,” Parikh adds. “There needs to be a seamless integration of mental health awareness across society. Equally important is the role of healthcare providers, sustained funding, and government policies. Only when these elements align can large-scale change become visible.”
Look how dark I was a few years ago, and look at me now,” said Archana Reena Shaikh, a 27-year-old transgender dancer from the Hijra community in Maharashtra’s Shrirampur city, as she scrolled through photos of herself on her phone. “It took five years for me to transform into the beauty you see today,” she said, speaking of her gender transition journey. Her face lit up as she spoke.
Hijra is a cultural identity in South Asia, involving trans, intersex and nonbinary people.
The difference between the Archana in the photos and the person sitting in front of me was stark. Her skin seemed smoother than before and she was definitely fairer—excessively so in fact, to the point of appearing pale.
The drastic transformation was the result of fairness injections that Archana had used—once every fortnight initially and then once a month—for nearly a year between mid-2023 and 2024. The key ingredient in the injections is an antioxidant called Glutathione, which is sometimes marketed as a “wonder drug” with skin-lightening properties.
According to the National Cancer Institute, Glutathione is naturally produced in the liver and by aiding in the process of detoxification, it helps protect the body from damage caused by toxins, ageing, and pollutants. It is widely used in skincare products since it is considered effective in preventing tanning and other kinds of skin damage caused by the sun.
Cognitive Market Research, a Pune-based market research and consulting firm, noted in its 2025 report that the Indian market for Glutathione was worth 13.39 million dollars in 2024 and is projected to grow at 12.7 percent annually over the next five years.
For Hijra women like Archana, Glutathione holds a particular appeal. As they transition to align their bodies with their gender identity, they say that the beauty standards set by Bollywood and popularised by social media shape their idea of the feminine ideal. Driven by the desire to be accepted and perceived as women, many of them end up chasing the flawless, glowing fair skin epitomised by their favourite actresses. And in the process, Glutathione injections become an integral part of the lives of some Hijra women.
Hijra women are not the only ones taking these injections though. From Bollywood celebrities to ordinary brides, the usage of Glutathione seems to have become so commonplace that it has begun to feature in the storylines of TV shows such as Made in Heaven.
These treatments, which are unregulated and often performed by unscrupulous clinics indulging in predatory practices, can pose health risks and come at a significant financial cost. The results can be unpredictable and begin to fade sometime after the user stops taking the injections. Yet, they seem to have become a trend.
Ease of Access
A few months ago, Taniya Khatun, a hijra woman who also lives in Shrirampur, made a phone call to a clinic in Pune to ask about fairness injections. Taniya recalled a soft-spoken voice answering her call, telling her to visit the clinic whenever she was ready. “We can start the treatment immediately, on the same day,” she said she was told.
“I was already fair, the same as you see me now,” Taniya told me. Yet, she travelled almost 200 kilometres to the clinic in Koregaon Park, Pune to seek treatment. “I took the injections due to peer pressure. It has become a trend [in her community],” she said.
The process was fairly simple. Taniya recalled that when she walked into the clinic, the staff asked for her budget and based on that selected an injection from a range of options. Then, she was told to lie on a bed and hooked up to an intravenous saline drip which contained Glutathione. Once the drip was finished, she said she was charged Rs 3000 and sent on her way.
The only instruction she was given was that for the injection to be truly effective, she needed to avoid exposing her skin to the sun and pollution for too long. Taniya, who is dependent on begging and dancing at public functions for an income, had to mostly ignore the directive. Maybe because of that, she said, she did not notice any change in her skin colour. She went back to the clinic for one more injection after the initial one.
Taniya’s experience is in line with medical knowledge of Glutathione’s effects. “It is a very slow-acting drug so it takes time for it to show effect. You will start seeing noticeable changes in colouration if you take it for the whole year, with the periodicity of an injection every three weeks,” said Shashank*, a dermatologist who works at two private hospitals in the National Capital Region. “But there is no guarantee that the fairness you achieved will last after that. We have seen the older colouration return after 3-4 months if patients stopped taking the injections.
Unlike Taniya, Archana persisted with the injections for much longer, taking 15 in total over the year. But when she stopped taking them, the Glutathione glow started to fade away. “I was even fairer than what you see now. The effects have reduced 50 percent,” she said with a hint of disappointment. Archana had spent Rs 53,000 on the treatment. That is roughly five months of income for her. She said she makes about Rs 10,000 a month through dance performances and begging.
The Hijra women I spoke to in Shrirampur told me that a two-person dance show typically earns them a total of Rs 2,000, while a four-person group performance might bring in Rs 5,000, exclusive of travel costs. Tilotama Patil, a 34-year-old Hijra woman who also lives in Shrirampur, said the Hijra women in her community are only able to get shows twice a month. They rely on tips to bolster their earnings, but Taniya told me that people often do not tip.
Almost all the Hijra women I spoke to for this story said that fairness treatments are becoming a financial burden for them. “We are left with no balance between how much we invest in our bodies and how much we earn. Fairness treatments alone cost more than what we make through dancing,” said Tilotama.
Unregulated and Unsupervised
Glutathione was never meant to make people fair,” said Shashank. “It was an accidental discovery. When doctors were using it to treat patients for liver conditions, they noticed a change in the skin colouration of patients. That is how it came to be marketed as a fairness drug.”
The Central Drugs Standard Control Organisation, India’s national regulatory body for cosmetics, pharmaceuticals, and medical devices, has only approved Glutathione for use in the treatment of liver-related diseases. However, hospitals and clinics across the country now offer it as a treatment to increase fairness and improve skin quality. The drug is also available in tablet and gel form, but injecting it is considered the most effective method to get immediate results.
“From big pharma to small drug manufacturers, everyone is making it. From big hospitals to small roadside clinics, everyone is injecting it,” said Shashank. “Around 2021, when my dermatologist friends and I started providing this treatment, we’d get about 5-6 patients in a month. But now, some of my friends are injecting Glutathione to 3-4 patients every day in Delhi NCR.”
Since its usage as a skin treatment is not officially approved, how it is administered varies wildly from one dermatologist to the next. “There are absolutely no guidelines. No dosage recommendations, no idea about how long it should be given and what is safe or unsafe. People are using it based on their whims and fancies,” said Shashank.
To get a first-hand experience of how easy it is to access Glutathione IV treatment and how predatory the clinics can be, I called up a clinic near my home in Salt Lake, Kolkata and made an appointment. While I was on my way I got three calls from the clinic in 20 minutes to know how far I was.
After I arrived at the clinic, I was then taken into a small chamber where a woman in her late 20s began suggesting fairness treatment options, including Glutathione injections. There were three options for the Glutathione injection — basic, advance, and premier. The basic option would involve 600 mg dosage per injection and cost Rs 36,000 for 15 sessions, advance was 20,000 mg for Rs 48,000, and premier was 90,000 mg for Rs 84,000. The main difference among them, she said, was that the injections with higher doses would lead to an “overall better effect on the skin and health.” When I asked about the side effects, she said, “It is completely safe.” The clinic staff was keen that I start the treatment right away. When I attempted to stall, saying I needed to think about it and discuss the cost with my family, the clinic manager offered discounts as well as EMI options which could be approved in 10 minutes flat.
For those who don’t want to deal with the cost of accessing it through a clinic, procuring Glutathione online is scarily trivial. When I googled “order glutathione injection,” a long list of corporate pharmacies and e-commerce websites showed up, promising to deliver Glutathione vials, in a variety of dosages and prices. Within 10 minutes of sharing my phone number with the e-commerce directory, Just Dial, I received messages from multiple vendors offering to ship the injections to my home.
“In our community, we see that people have started purchasing these injections online and injecting it with the help of nurses who can implant an IV either at home or at local clinics,” said Tilotama. Multiple Hijra women I spoke to in Shrirampur said that this helps them not only cut the cost but also gives them the freedom to take higher doses. Their reasoning is that higher doses, taken more frequently, mean quicker, more effective results.
This kind of unregulated and unsupervised use of Glutathione injections can be harmful. The US Food and Drug Administration warned in a 2019 advisory that potential side effects from Glutathione injections could include harmful impacts on the liver, kidneys and nervous system.
Rashmi Sarkar, Director Professor at the Department of Dermatology, Leprosy, and Venereology at Lady Hardinge Medical College and Hospital, told me that while topical and oral Glutathione are relatively safer, they should not be used indiscriminately without a dermatologist’s advice. The intravenous injection of the same drug is a “strict no because of the side effects.”
“We don’t know in which way it will work. The results can be unpredictable and the procedure can lead to severe side-effects. It can have renal side effects, severe skin reactions, sometimes it can lead to peeling of the entire skin,” she said. Adding that these side effects don’t occur all the time, she emphasised that due to the lack of clinical trials involving Glutathione injections, doctors are flying blind with regard to potential risks. Shashank, however, said that none of his patients ever had any side effects.
In an article published in The Print, Deepali Bhardwaj, a dermatologist and aesthetician, wrote, “Glutathione affects your kidney function in the long run. You need to know what dosage works for you. And you will need to first take a kidney test to see the viability of administering the glutathione injection.” Both Archana and Taniya told me that they were neither asked to undergo any tests before or after taking these injections nor were they told about any potential side effects.
The potential risks do not seem to faze Archana though. “We do not care about the side effects. Most of us live a short life, we rather live it satisfied,” she said firmly.
The Emotional Burden
The quest for fair skin can also have serious implications for the mental health of Hijra persons.
In a 2020 study, 38 percent of Hijra persons reported having some kind of mental health condition. These challenges, the studies note, are systemic and often stem from societal stigma, discrimination, rejection by family and friends, violence and lack of access to appropriate healthcare services.
For the Hijra women of Shrirampur, pre-existing mental health pressures are exacerbated by society’s emphasis on conventional beauty standards, and sometimes lead to a deep sense of isolation and despair.
“For a Hijra woman, it is important to look like a woman. And the image of a woman is all about fair skin, a thin waist, long hair and pink, puffed lips,” said Tilotama. The goal, as she puts it, is to escape the popular imagination of a Hijra woman as “someone with dark and heavy makeup, whose face is packed with layers of foundation that do not match the rest of her body.”
But the quest for acceptance through fair skin among the Hijra community isn’t confined to Shrirampur. Yoga S. Nambiar, who has a PhD in mental health and is the founder of the Global Rights Foundation, an Ulhasnagar-based NGO focused on transgender welfare, said that the phenomenon is widespread. “I can vouch for Delhi, Maharashtra and Punjab and say that around 45 percent of community members are taking these glutathione injections and also pills,” she told me.
This struggle does not end at fair skin but leads them to other treatments too. “From skin whitening treatments to lip fillers and liposuctions (cosmetic fat removal surgery) too, almost all of us save for years to get these procedures done,” Tilotama said. “It is not just about becoming fair, it is about finding self-acceptance.”
From Screen to Skin: the Media’s role
Tilotama sees having fair skin partly as a professional requirement—being perceived as attractive helps Hijra performers get more shows.
It has been 17 years since Tilotama started her gender transition journey. Now 34, she has never taken a Glutathione injection, nor does she wish to take one because she believes she is already fair. She said she can maintain her skin tone by using fairness creams. Tilotama believes that the aggressive marketing of fair skin tones through social media and films is the main reason driving this generational shift.
“Earlier, Hijra women from our community would follow heroines like Kajol and many like her who were not fair; the darker shades were appreciated more back then,” said Tilotama. Kajol, a Bollywood actress who debuted in the early 90s, has spoken of how she was taunted for being dark in her early days in the industry. Her skin has become markedly fairer in the decades since. While she denies using any skin treatments, attributing her fairness to “staying out of the sun,” other Bollywood actresses and social media celebrities are quite open about the treatments they use, including Glutathione.
These kinds of cultural shifts are forcing some Hijra performers to adapt even though many of them may not be able to afford such treatments. Outfits once inspired by traditional, conservative styles have been replaced by revealing costumes: blouses with thin bra-like straps and skirts with thigh-high slits. “Our livelihood depends on adapting to these trends,” Tilotama said. “If we don’t, we’re left behind or forced to perform [only] in rural areas where the pay is significantly lower.”
As a result, Hijra women in rural places like Shirampur find themselves striving to embrace a beauty ideal that can be unattainable or damaging.
Tilotama described to me how when a dancer from a city is hired in their small town, she brings the city fashion with her. After that, she said, audiences only want to see dancers who resemble them. In order to compete, women like Taniya and Archana sign up for endless procedures and treatments to alter their bodies.
“If you open a shop or a parlour, if you decorate that shop and invest in it then only you will be able to attract customers, right? Similarly, we need to invest in our bodies and look pretty, then only we can get work. After all, people only care about outer beauty and not skills anymore,” Tilotama explained.
In Yoga’s opinion, the pressure to be fair comes not just from professional compulsions, but also from wanting to be a desirable romantic partner. “I think transgender people are taking Glutathione because the livelihoods they are dependent on like badhai, toli or begging involve a lot of exposure to the sun, which makes the skin dull. But the general expectation is to look good and attractive so your boyfriend will love you more and stay with you,” she said. “Hijra women really believe that if they start looking more and more like a [cis]woman their boyfriends will come back to them. But, honestly, nothing of that sort happens, boys come, have fun and then leave.”
“There is no shortcut to self-acceptance, one needs to seek support from supportive individuals,” said Meenal Solanki, a Delhi-based counselling psychologist. She believes that the journey towards self-acceptance for Hijra women like Archana needs to include a collective, community-based approach.
“For a queer person, I feel social support—finding your people, other queers, a sense of community—is extremely important,” she said. “Receiving compassion from or even being around queer individuals, who are vibrantly themselves in all their shapes & sizes, who model self-compassion, will be super helpful for queer individuals to fast track self-compassion, along with working in therapy.
But the path Meenal is prescribing is less straightforward than the one offered by skin clinics eager to add to their bottom line.
“Tomorrow is my ex-boyfriend’s marriage and on this occasion, I have decided to put my entire efforts to be prettier than his wife,” Archana’s voice echoes.
Having taken a six-month break, Archana is now planning to start taking Glutathione injections again. She wants to invest whatever spare money she has in beauty and has no plans of saving up for old age.
“My last wish is to die fair and pretty, there is nothing else to this life,” she said.
A report by the World Health Organization (WHO) and International Labour Organization (ILO) revealed that long working hours were responsible for thousands of deaths from stroke and heart disease, with a large number occurring in Southeast Asia and the Western Pacific region. The rise in fatalities linked to overwork reflects a broader trend in Asia, where burnout is often accepted as the cost of success. These figures don’t even include rising suicide rates from excessive workplace pressure, highlighting the grim reality of sacrificing physical and mental health for career achievement.
Illustration: Sharanya Eshwar
In India, 26-year-old Anna Sebastian Perayil tragically died just four months after joining one of the world’s leading accounting firms. The cause? Overwork, exhaustion, and burnout. She pushed herself beyond her limits, driven by the hope for a better future — a promise we’ve all been sold: “Work hard now, so you can relax later.” But when does this elusive “later” ever come? For Anna, like many others caught in the grind of toxic hustle culture, that moment of rest never arrived. Instead, she became another victim of a system that prioritises profit over people, perpetuating the myth that success is worth sacrificing your health.
The Japanese have a term that describes such deaths: “Karoshi”, which means “overwork death”. This refers to loss of life or an impairment caused by overwork which was the case with Miwa Sado, who was a journalist from Japan and died due to burnout. The Koreans term this as ‘Gwarosa’ which also means death by overworking. The praise and glorification of endurance to prioritise delivering consistently over well-being traps employees in a cycle of overwork and exhaustion, which often lead to tragic consequences. The “996” work culture in China demands employees to work from 9 AM to 9 PM, six days a week, or 72 hours a week. Employees in China, especially in the tech industry are bombarded with relentless expectations of availability and productivity, with little room for rest or personal time. Research shows that about 600,000 Chinese people die every year because of “Guolaosi” – death by overwork.
Anna Sebastian’s mother’s letter to her employer after her death highlights the painful reality of how employees become disposable. Her grief is compounded by the fact that no one from Anna’s office even attended her funeral, reflecting the dehumanising nature of corporate culture. In South Korea, families facing similar losses not only endure emotional pain but also legal struggles to prove death by overwork (Gwarosa). This adds financial strain, leaving them to bear the burden of losing both a loved one and a primary breadwinner.
In Asia, hard work isn’t just encouraged—it’s a way of life. From early childhood, students face immense pressure to excel in highly competitive environments and prepare for cutthroat exams that determine their future. Securing a job in an unforgiving market is the next hurdle, but it doesn’t end there. These challenges serve as training grounds for the relentless pressure, long hours, and uncertainty that dominate the workplace. The culture of striving for success, combined with societal expectations, conditions employees to accept stress as a norm, blurring the lines between dedication and self-sacrifice. This pervasive mindset shapes not only individual behaviour but the entire work culture across Asia.
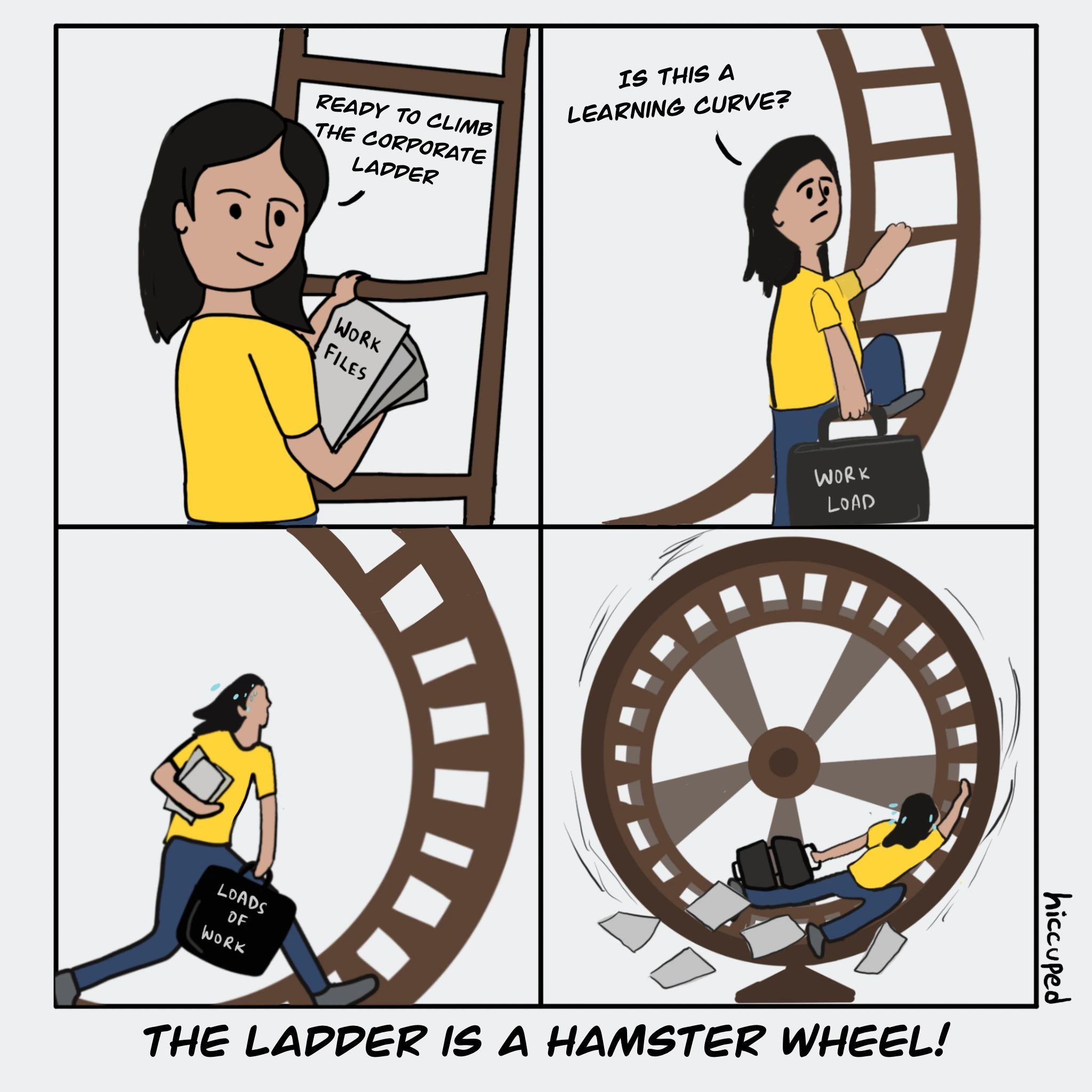
We are conditioned to celebrate overwork and to glorify burnout as a form of ambition. The concept of “work-life balance” is merely an illusion, as the line between work and personal life has become increasingly blurred. Terms like “grind” and “hustle” have infiltrated our vocabulary and subconscious, tricking us into believing that working overtime is a heroic endeavour. In a capitalist setting, even the death of an employee due to burnout will only prompt the HR to “touch base” on the importance of mental health, so together they can “synergise” and “recalibrate” strategies that will then turn to “circling back” on some wellness initiatives and maybe plan a team-building activity that will quietly fade away due to more deadlines. In the end, nothing really changes — just a lot of words designed to “move the needle” on corporate image, but not much for the employees.
Rosa Luxemburg once said, “Those who do not move, do not notice their chains.” This is true in the context of today’s toxic work culture. We often fail to recognise the invisible chains that bind us to the sense of false belief that hard work must mean overwork. It’s time to break away from this notion. True progress isn’t about pushing ourselves to the brink—it’s about knowing when to pause, prioritise our health, and reclaim our well-being from a system that too often exploits us.